
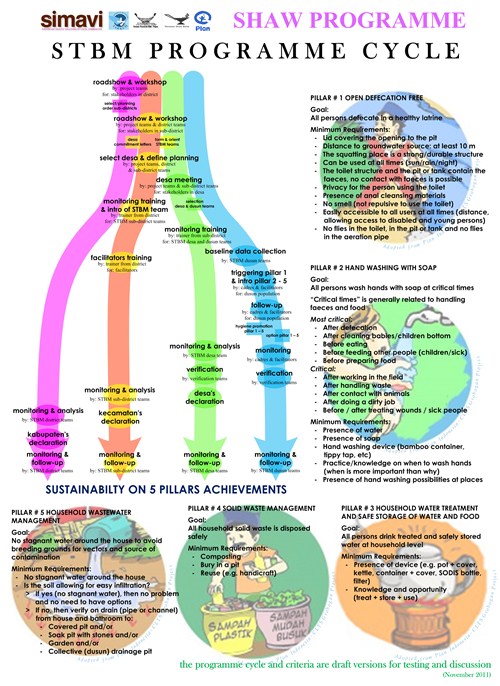
The SHAW project (2010-2014) was created to promote and facilitate a national strategy called Community Based Total Sanitation, or STBM in Indonesian, based on the Community-Led Total Sanitation (CLTS) approach. The central focus of the STBM strategy concerned sustainable behaviour change towards health. The STBM strategy had 5 pillars: Open defecation free; Handwashing with soap; Household water treatment and safe storage; Solid waste management; and Household wastewater management.
I worked on the SHAW project as the coordinator from the inception period in 2010 up to almost project closure end of 2014. Previously, I worked in the WASH sector, including on CLTS projects with Robert Chambers, in several countries in Africa, and had learned how to facilitate the CLTS approach.
The SHAW project aimed to include within the STBM strategy: 1.5 million persons in 5 islands, 9 districts, 114 sub-districts, 1042 villages in Eastern Indonesia. Attention to school sanitation and water supply was included. The major objective of the SHAW project was to get a sustained 100% STBM coverage in as many villages as possible (it had a rural focus), and hopefully 100% STBM coverage of sub-districts. Another objective was to develop a general approach to sustainable STBM, to be used by government and NGOs.
From the start, activities were focused on long-term sustainability from my firm belief that a project is just an initial stage, and the population must continue the work, supported by the government and local organisations. From the outset, close contacts with government institutions were established at national, district, sub-district as well as village level.
I facilitated a learning-by-doing process to refine the initial approach, while ensuring that it became a framework approach, leaving space for details. After all, each area and every village has its own characteristics.
Why share learnings now?
I didn’t write this blog earlier for to several reasons (among others my health) but even though nine years have passed, I feel lessons from the project are still relevant today. The main learnings I want to share are around the approach that was used and how it was adjusted successfully during the project. The fact that it achieved behaviour change in up to 1.2 million people adopting ODF practices [1] is very significant yet very little has been written or shared to the wider WASH sector about this project’s process, findings and outcomes. Throughout this blog I reference SHAW project resources, which are available in the reference section at the end.
What made the SHAW project successful?
Below I outline some of the key elements that made the SHAW project successful:
Convening and facilitation of stakeholders
Participatory approaches to convening and facilitation (developed from CLTS) at various stages of the project, with various groups, were essential to its success.
Facilitating governments, INGOs and donors
The SHAW project discussed at several moments its approach, the results and way forward with government (national, district and sub-district), international organisations (a.o. WSP, UNICEF, SNV) and the donor (Netherlands Government). The aim was to obtain a widely supported approach as well as broad information sharing and updating.
Key consultation moments:
- First in 2010 after an inception period, resulting in a working plan.
- Second moment was a review end 2011 with field visits and a workshop to discuss the approach and results so far and advise on the next steps.
- The third moment was a similar review mid-2013, to verify the results and discuss how to ensure sustainable results. During the review, (sub-)district officials went to other islands as an exchange.[7]
- The official mid- and final evaluations took place in 2012 and 2014.[1] They were formulated by the donor and national government and realised by independent experts. The evaluations were broadly discussed, also to agree on next activities.
Facilitating INGO and local NGOs
The project was implemented by 5 Indonesian NGO’s and one coordinating international NGO, with support by IRC-WASH. Each Indonesian NGO was operating on a different island in Eastern Indonesia, and was well established, including contacts with the villages and at government levels. Each NGO started off along its own characteristics during 3 months. After this inception period and with the working plan (2010), an overall approach was agreed upon.
All NGO’s met each quarter to discuss progress, problems and way forward. When needed, adaptations were introduced. Government staffs sometimes joined these quarterly meetings. At national level, the progress and eventual adaptations were regularly discussed with the ministries and donor, to inform and obtain their continued support.
Facilitating at district level, sub-district and village level
When starting in a district, the STBM decree was elaborated with district officials into an approach on how to operate and what would be the roles. Key during the discussions was that the district was responsible to implement the national STBM decree and during its term, the project could facilitate the process. The same meetings took place at sub-district level.
Then, a meeting was organised by the sub-district leader for all village leaders, to introduce the objective of STBM, and discuss steps forward. An expression of interest was signed by the village chiefs. Some villages did not sign, reluctant to be responsible for implementing by themselves without receiving cash or tools. A key part of the approach was that investments were to be made by the target population, not by others.
Sub-district staff(s) and SHAW NGO staff visited each village that had expressed interest, to introduce the subject and, if they were still interested, discuss how they could support and facilitate the villagers on implementing the different pillars by themselves. The SHAW staff returned several times to the same village as follow-up and support to their STBM activities. Government staff did not always join them. Several at first reluctant villages later solicited SHAW to come and assist them, when they observed the enthusiasm and the positive impact at neighbouring villages. Also, villages asked neighbouring villagers to train them in the how to.
Some important rules for the SHAW staff concerned to not act as an all-knowing person from outside but discuss (talking, not telling), their experiences and opinion are the starting point. Another rule was to show respect and keep your promises.
Generally, women were the first to understand the benefits for the family, and took initiative, motivating the men to make the constructions.
Recommended by the first review was to take up STBM at schools and involve more the private sector, religious and community-based organisations.
Participatory monitoring
The SHAW project introduced an extensive step-wise monitoring programme [3]: the villagers collected quarterly the information, with the village leader to consolidate the village data. The SHAW NGO consolidated the sub-district data and submitted the report to the sub-district officials. The sub-district data were submitted to the district officials. The last step was to consolidate the data of the 9 districts and submit the report at national level (Ministry of Health and Ministry of Planning) and the donor. Each government level was hence quarterly informed on progress, giving opportunities to intervene if deemed necessary.
The monitoring system itself was set-up to cope with illiteracy at village level. Drawings helped the observer to indicate the situation per household for each pillar (improved yes/no). Each quarter, mainly women passed effectively house by house, and gave advice when the situation was not appropriate. During the follow-up visits, SHAW staff also monitored the quality of the data.
Some sub-district leaders became so enthusiast by the positive impact (see below) that they joined the promotion team at some stages.
A ceremonial step was introduced by SHAW to celebrate when a village reached 100% STBM. The ceremony was commonly done by the sub-district leader. But sometimes the district leader headed the ceremony, especially when a whole sub-district reached 100% STBM. Once, the Minister of Health joined a 100% STBM ceremony. A 100% STBM ceremony was strictly ceremonial, there were no rewards.
What did success look like?
By mid-2014, monitoring showed that the number of inhabitants respecting the STBM behaviour varied between 0.97 to 1.3 million persons per pillar (66 – 91% of the target population). Also, 456 Schools observed 100% STBM (85% of the target).[1]
An impact study was conducted to apprehend the perception by the villagers, teachers and government officials on the benefits [6]. The perceived benefits were at:
- Village level: clean living environment, health improvement, time saving, more household income (including savings from less medical costs), education and childcare, collaboration in community (including assistance to the poor), self-esteem and a more comfortable life.
- School level: improved school attendance and performance.
- Private sector: income from toilet slab production.
- Government level: in control of health improvements in their (sub-)district, more time for activities outside health, self-confidence and pride as model for learning STBM.
By mid-2014, the overall expenditures were at €16.6m, contributed by the donor 41%, local government 9%, participating NGOs 9%, and the villagers 41% (estimated investment costs).
In 2014 the Indonesian Ministry of Health issued regulation number 3/2014 concerning an updated implementation strategy of STBM [2]. The approach described was largely inspired by the approach by the SHAW project.
What were the challenges of this approach?
Several challenges surfaced during the project:
- Developing and refining the approach for 5-pillar STBM in a participative way took much time and efforts.
- The approach worked well in villages, with their sense of community. But STBM in towns got no attention since it required another approach due to less community sense.
- Information sharing beyond the mentioned group dropped behind: Some townspeople wanted to copy the ideas, but information lagged; Uploads to generate wider interest lagged. Issue was a focus to give substantial information which was only available at the end, too late.
- The monitoring scheme worked well during the project but needs to be adjusted to work after the project, it was too complex and expensive.
- A major challenge was to motivate government institutes to allocate staff time and budget to participate, leave alone to lead the STBM process. Also, the level of understanding varied.
Has this success sustained?
By mid-2015, STBM had touched 1.45 million persons and 802 villages were declared 100% STBM. Between 2016-2019 a follow-up project called SEHATI (Sustainable Sanitation and Hygiene for Eastern Indonesia) was implemented which built on the success of the SHAW approach. In 2019 the SEHATI team produced guidelines for local governments to replicate the SEHATI approach to other villages or sub-districts that had not been reached by the programme. Unfortunately, the resource does not mention STBM achievements at this point, nor does it provide an update on the original SHAW districts.
What are the next steps?
As the learning from the SHAW project has not been widely acknowledged or shared, please find links below to reports available from the project. The hope is that this information will be of value to other WASH professionals across the sector. If you require more information please contact me [email protected]
SHAW project references
1. Febriani, E., Sukarma, R., Van Esbroeck, D., Ferdy, H. Y and Frans, N. [external evaluators] (2014) End Evaluation of the Sanitation, Hygiene and Water (SHAW) for East Indonesia project: Synthesis report.
2. The Ministry of Health Republic of Indonesia (2014) Republic of Indonesia Hygiene and Sanitary behaviour within the Community-Based Total Sanitation. Regulation of the Ministry of Health on STBM.
3. SHAW project (2014) Visualisation of the SHAW monitoring programme
4. SHAW project (2014) SHAW Flow of activities
5. SHAW project (2014) Progress Report January–June 2014
6. SHAW project (2014) Study on perceived 5 Pillars STBM behaviour change
7. SHAW project (2013) Joint review meeting, “Building Partnerships for Sustainability” 17-18 June 2013, Jakarta, Indonesia
8. Minnigh, P. and M. Keijzer, M. (2014) The SHAW Experience in Indonesia: The multi-stakeholder approach to sustainable sanitation and hygiene. Briefing paper: 37th WEDC International Conference, Hanoi, Vietnam, 2014
[Photo caption: Producer of concrete toilet slabs, generating income. Some producers used different colours to make the slabs more attractive. Flores May 2014. Photo credit: Martin Keijzer]





{kind=link}